 Endometriosis is a condition in which endometrial tissue that is still functioning, are outside the uterine cavity. This tissue is composed of glands and stroma, myometrium contained in or outside the uterus. When endometrial tissue present in the myometrium is called adenomyosis, and when outside of the uterus is called endometriosis.
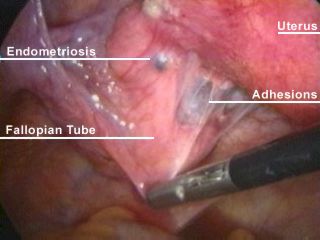
Endometriosis is a condition in which endometrial tissue that is still functioning, are outside the uterine cavity. This tissue is composed of glands and stroma, myometrium contained in or outside the uterus. When endometrial tissue present in the myometrium is called adenomyosis, and when outside of the uterus is called endometriosis. In endometriosis, endometrial tissue is found outside the uterine cavity and the outer myometrium. The areas most commonly affected are the pelvic organs and peritoneum, although other organs such as lungs also affected although rarely. The disease is evolving from a small lesions and a little on the pelvic organs are normal then a hard mass infiltrates and cystic ovarian endometriosis (endometrioma). endometriosis is often accompanied by the formation of extensive fibrosis and adhesions cause pelvic anatomy.
ETIOLOGY
The cause of endometriosis is still unknown. Several theories emerged regarding anatomical factors, immunological, hormonal, and genetic.
1. Retrograde menstruation.
According to Sampson, endometriosis occurs because of menstrual blood to flow back (regurgitation) through the tube into the pelvic cavity. Already proved that menstrual blood was found in endometrial cells are still alive. Endometrial cells surviving implantation can then be entered in the pelvis.
2. immunological factors
Specific immunological factors that play a role in the implantation of endometriosis such as VEGF (vascular endothelial growth factor), MIF (migration inhibitory factor), and inflammatory mediators (interleukins, TNF) is suspected to have increased at the site of endometriosis.
3. hormonal factors
Aromatase, an enzyme triggers the production of estrogen, has been found on the implantation of endometriosis, although not yet found data that aromatase is also found in normal endometrium. PGE2(prostaglandin E2) serves as the strongest induction of aromatase production in endometriosis implantation.
4. Celomic metaplasia
Theory suggests the potential of cells in the ovary and peritoneum transformed into endometriosis lesions caused by hormonal stimulation of hormones and repeated exposure. Robert Meyer suggests that endometriosis occurs due to stimulation of the coelomic epithelial cells that can sustain life in the pelvic area. This stimulation causes metaplasia of epithelial cells, thus forming endometrial tissue.
5. deployment limphatic
A study of autopsy showed that endometriosis cells are found in the pelvic lymph glands in 29% of women. This may explain why endometriosis ever found in the lungs.
6. genetic factors
Women who have a family history of endometriosis, a seven-fold risk of suffering from endometriosis. Undiscovered genetic defects in endometriosis.

RISK FACTORS
Risk factors include age, increased number of peripheral body fat, and menstrual disorders (polimenore, menorrhagia, and reduced parity). Smoking habits, exercise, and oral contraceptive use may be protective. There has been no evidence to suggest that controlling the risk factors can prevent the appearance of endometriosis. Genetic factors play 6-9 times more with a history of immediate family suffer from endometriosis.
CLINICAL SYMPTOMS
The symptoms are often found in this disease are:
1) under a progressive abdominal pain and thigh that occurs close to and during menstruation (Dysmenorrhea);
2) disparenunia;
3) painful defecation time, especially at the time of defecation;
4) poly-and hypermenorrhea;
5) infertility.
Dysmenorrhea in endometriosis menstrual pain usually is gradually increasing in intensity. Cause of dysmenorrhea is unknown, but probably something to do with vascularization and hemorrhage in the nests of endometriosis at the time before and during menstruation. Pain is not always obtained, although abnormalities in endometriosis is extensive, should be mild abnormalities can cause symptoms of severe pain.
Dyspareunia is a common symptom, caused by the presence of endometriosis in the pouch of Douglas. A difficult and painful defecation, especially at the time of menstruation, caused by the presence of endometriosis on the wall rectosigmoid. Sometimes it can happen stenosis of the lumen of the colon. Bladder endometriosis is rare, the symptoms are impaired micturition and hematuria at the time of menstruation. Menstrual disorders and the cycle may occur in endometriosis when abnormalities in the ovaries so extensive that impaired ovarian function. There is a real correlation between endometriosis and infertility. 30-40 percent of women with endometriosis suffer from infertility. likely to become pregnant in women with endometriosis is less than half of the ordinary woman. An important factor causing infertility in endometriosis is when the mobility impaired due to fibrosis and tubal adhesions surrounding tissue. On gynecologic examination, especially in the examination vagino-recto-abdominal, are found in mild endometriosis, solid objects of grains of rice to the grain of corn in the pouch of Douglas and the ligament of the uterus in retrofleksi sacrouterinum with and fixed. Ovary at first be felt as a small tumor, but can be enlarged to the size of a fist. Ovarian tumors are often bilateral and driven hard.
DIAGNOSIS
The diagnosis is usually made on the basis of history and examination, confirmed by laparoscopy examination. Kuldoscopy less useful, especially if the pouch of Douglas participated in endometriosis. In endometriosis were found in locations such as the posterior vaginal fornix, perineum, laparotomy scars, and so forth, a biopsy can provide certainty about the diagnosis. Laboratory tests in endometriosis is not a typical signal, only when there is blood in the stool or urine at the time of menstruation is an indication of the existence of endometriosis in the rectosigmoid or bladder. Sigmoidoscopy and cystoscopy can show where bleeding during menstruation. Making plain by including barium in the colon can give a picture filling defect in rectosigmoid with clear boundaries and an intact mucosa. Laparoscopy is an examination that is very useful to distinguish endometriosis of abnormalities in the pelvis.
TREATMENT
When the diagnosis of endometriosis was established, treatment options taken based on the extent of endometriosis and the patient's needs. Regimen of oral medication and surgery are determined by age, fertility status, severity of illness, previous treatment, cost, risks of treatment, and duration of treatment. The purpose of this treatment are:
-What-treated (disease, symptoms, or both)?
- Why is administered therapy?
Provide therapeutic reasons: to restore fertility, as an alternative to surgery to relieve pain, relieve pain while waiting for surgery, prophylaxis to prevent recurrence of disease.
1.Terapi conservative
Endometriosis implantation has the same properties and reactions with the endometrium, especially in the production of estrogen. Conservative therapy aims to suppress the stimulation estrogenovarium to bypass the hypothalamic-pituitary-ovarian. Inhibition of ovulation with gonadotropins through a cycle of sex steroids can inhibit the formation of endometriosis.
a. inhibition of aromatase
Letrozole Anastrozole 1 mg or 2.5 md every day is a third generation aromatase inhibitor that inhibit the changes of androgens to estrogens by 50%. Side effects of this drug is a decrease in bone density, but this can be prevented with vitamin D and calcium intake.
b. pain control
Non-steroidal anti-inflammatory drugs (NSAIDs) inhibit prostaglandin released by endometriosis. NSAIDs are first-line drugs that are used when the diagnosis of endometriosis has not been enforced.
1. surgical therapy
Conservative therapy is a modality for patients who just want to relieve pain or to relieve pain in fertile conditions. For patients who are infertile, or patients who do not respond to conservative therapy, surgical therapy is an option. Surgery consists of definitive surgical therapy and conservatife.
1.Terapi definitive surgery includes total hysterectomy with bilateral salphyingo-ooferectomy. After definitive surgery performed, patients were given hormone replacement therapy
(Hormone Replacement Theraphy).
2.Terapi conservative surgery aims to restore the position of the pelvic anatomy and remove all visible endometriosis lesions.
COMPLICATIONS
When implantation occurs in the intestine or ureter may lead to obstruction and impaired renal function. Pelvic distortion resulting in impaired fertility, oral contraceptive use resulted troboembolisme hipoetrogen effects of GnRH analogues and long-term result of osteoporosis.
PREVENTION
Medical Shaman argues that pregnancy is the best way to prevent endometriosis. The symptoms of endometriosis are reduced or lost during and after pregnancy because endometrial regression in the nests of endometriosis. Therefore, marriage should not be delayed too long, and after marriage should be sought so that a desired children in the not too long. Such an attitude was not only a good prophylactic against endometriosis, but avoid the occurrence of infertility after endometriosis arise. Also do not perform inspections or conduct rough scrapings during menstruation, because it can cause the flow of menstrual blood from the uterus into the tube and into the pelvic cavity.
jujur saja tidak mengerti tentang hal ini, tapi ikut nyimak aja .......
ReplyDeletengerti ga ngerti yang penting saling komentar di postingan, di tunggu
ReplyDelete;p kurang faham.
ReplyDeleteBagus banget artikelnya, jadi kita banya tahu kiat untuk menghindari,mencegah serta cara mengobati penyakit,trims infonya gan
ReplyDeletewidihhh. jadin takut liat gambarnya,bagus artikelnya..makasi dah share gan
ReplyDeleteWah, blognya pke bhs Inggris jd harus hati2 bacanya. He
ReplyDeletea very complete article, hopefully can help many people
ReplyDeleteinfonya bagus sobbb... lanjutkan..
ReplyDeleteThis is an informative overview about endometriosis.
ReplyDelete